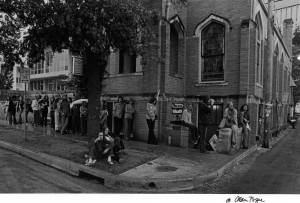
Everyone seems to know the creation story: People’s Community Clinic began in the basement of the Congregational Church of Austin in 1970. It was a humble operation. A few evenings each week, a volunteer staff of physicians and health providers delivered free healthcare to patients who otherwise couldn’t afford it. Patients wrapped around the side of the church waiting to be seen, and volunteer doctors and staff stood on the sidewalk shaking coffee cans for donations to keep the clinic afloat. This is not that story. This is the story of Reverend John Chesley Towery—the man who gave PCC its first home.
His story begins in Corydon, Kentucky five decades earlier. Towery was born March 25, 1926—the older of two sons who would one day become ministers. After graduating valedictorian of his high school class in 1943, Towery attended the University of North Carolina and joined its V12 Naval Reserve Officers Training Corp, an accelerated program designed to produce naval officers for the war effort. He was commissioned at graduation in 1946, and afterward served as an ensign on the USS Nantahala, a tanker that replenished fuel for ships in the Pacific theater.


One might think of the Nantahala as a service ship that played a support role as it delivered the fuel and cargo others needed to do their jobs. Crew members worked tirelessly as they traveled throughout Japan, the Philippines, the Malay Peninsula, and along the coast of China refueling ships. Although the war had ended during Towery’s service, the devastation from it had not. Viewing the damage likely influenced his career path, wrote longtime friend Mel Oakes.
Upon returning stateside he used the GI Bill to attend Yale Divinity School where he received his Masters of Divinity. He was ordained in 1950 and accepted a position as minister of the Mount Holly Christian Chapel in Amelia, Ohio where he met and married Eleanor Ruth Morgan that same year.
Together they served in churches in Ohio, Idaho, and Wyoming before a position opened at the Congregational Church of Austin in 1959. It would be Towerys final move and where their three children Joseph Chesley ‘Ches’, Sally, and Mary were raised. It was also where Reverend Towery pressed for his congregation and community to build a culture of involvement—regardless of the color of one’s skin, their sexual identification, politics, or poverty. For Oakes and his wife Pat, that message of welcoming others is what drew them into the Congregational Church in 1964. The Oakes moved to Austin from Tallahassee where they had stopped attending church in Florida due to unfair division. A visit to the Congregational Church of Austin proved different.
Reverend Towery worked to upend policies of division in Austin. He demonstrated against separation in movie theaters in Austin. He drove to Huston-Tillotson University each week to invite students and faculty to attend church services—actions that would later prompt the university to award him with an honorary doctorate for his involvement in the civil rights movement.
“John had a special affinity for those people who were closed out of society,” Oakes said during a recent memorial service for the reverend. “John opened the church’s doors to troubled youth and invited them inside to be cared for in a ministry called The Raft. And through his personal involvement in the civil rights movement, his personal commitment to bring the people of Austin together, John helped open up the doors that were closed to people because of the color of their skin.”
As a child, Mary Towery, now Mary Masters, didn’t realize the impact her parents had on their church and their community. Part of it is because Reverend Towery was her father, and partly because he and her mother lived what they preached. Her dad had the ability to challenge social stances without being confrontational; he had a soft touch that was effective when dealing with hard issues. And they operated as a team. Just as her father helped push through programs in the church like the Raft, it was because he had his wife’s support and energy to do it, Masters said.
Her parents approached the world with open arms and hearts. They impressed upon their children the importance of fairness and openness, she said. “It wasn’t just something they preached form the pulpit on Sunday. They lived it.”

The Towerys applied the same open door policy to their home as well as the church. Occasionally the family took in people who needed one. Part of this is likely the influence of her mother, a foster child herself, Masters said. Sometimes for the Towery children this meant sharing rooms as well as a home.
“I don’t remember it being hard because it was always filled with love,” Masters said.
After starting the Raft program, which provided shelter to homeless teens who needed it, Reverend Towery offered did the same for those who needed healthcare. He saw that people in the community were in need and offered the basement of the church to the People’s Free Clinic who were working to address it.
“He was the type of minister who felt that the church should not just be used on Sunday,” Masters said. “My father fought very hard for [the clinic] and wanted it to be a success. He never dreamed that it would outgrow the church, or outgrow the clinic where you are now.”


Growing up, Masters often helped clean rooms in the church for potluck events and would open the refrigerator to find it stocked with medications and syringes as well as leftovers. Sunday school rooms were flanked by examining tables stashed behind curtains.
“It was all so fascinating to me,” she said. “It was the real world and as Christian it made you realize that this is what it’s supposed to be about.”
Alicia M. Jarry, one of PCC’s earliest volunteer providers, recalls how Reverend Towery’s invitation to house the clinic in its basement allowed thousands of people, including pregnant women and homeless individuals, access to care.
“I remember so clearly his involvement in expanding our services and allowing us to use the upstairs sitting area to have counselors give health information and advice to those who could not receive it elsewhere,” she said. “He was part of the health care team that included many doctors and nurses who worked as volunteers or for low wages to serve this population.”
And his impact on PCC continues today. One impressionable 8-year-old never forgot the lessons she learned in the Towery household. Robin Rosell, PCC’s director of social services, was childhood best friends with Mary (Towery) Masters. Reverend Towery used to drive the girls to middle school events and later to high school football games. He was a master gardener and had a plot in one of the city’s community gardens. He routinely sent friends and neighbors home with fresh produce.
“He planted literal seeds and so many other seeds that are continuing today,” Rosell said.
Towery was the type of person who didn’t assume a locked gate meant no entry, he just looked for another way over. And when he spoke, Rosell listened.
“I heard him tell the stories of the very beginning [of People’s Community Clinic],” she says from her office on the clinic’s second floor overlooking I-35. “He always talked about People’s. He was very proud of what had started there … He was a bit of a Renaissance man. I think growing up watching somebody who put his beliefs into action and did so much good in the community, it was inspiring. I thought that is the type of person I’d like to be.”

She remembers the lines of people waiting to be seen at the clinic, when Lucinda Williams still played on the drag. In PCC’s early days there was no air conditioning, there weren’t even exam tables available. Over time, the clinic acquired an air conditioning unit and eventually grew so large it had to move out of the church basement. Rosell grew up too.
She studied special education teaching and later social work as a graduate student at UT Austin. If she had a hard day she headed for the Towerys. And she never went to the front door. She knew the couple would be sitting in the back of the house and head straight for it.
Nearly 19 years ago Rosell saw a job posting in the newspaper seeking a social worker at a “fast-paced community clinic.” There was no name listed for the clinic. She applied anyway. When Rosell was called for an interview she learned it was at PCC. After being offered the job she picked up the phone.
“The Towerys were the first people I called,” Rosell said smiling. “It kind of felt like I had grown up.”
Reverend Towery led the Congregational Church for 30 years. He died November 28, 2014. Eleanor passed away March 3, 2014. They were married 63 years. A celebration of Reverend Towery’s life will be held January 18 at 11 a.m. at the Congregational Church of Austin located at 408 West 23rd Street.
-KM